
Reading time: 4 minutes
Indiwari Gopallawa
Cancer is the second leading cause of death after cardiovascular diseases in the United States and has a major impact on society. Lung cancer is the second most common cancer type and is associated with lower survival rates and higher cancer-related deaths, accounting for 25% of all cancer-related deaths (https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics).
What is Non-small cell lung cancer?
Non-small cell lung cancer (NSCLC) and small-cell lung cancer (SCLC) are two major lung cancer types. NSCLC is the most common type, accounting for about 80% – 85% of all lung cancers. It progresses more slowly compared to SCLC.
Like many other cancers, NSCLC begins when a lung cell (the smallest structure of the lung) changes or mutates. Cells contain genes that provide instructions for cell growth. Changes or mutations to a gene can cause cells to grow too large. These changes within cells can occur when they are exposed to dangerous chemicals such as carcinogens. However, sometimes the exact cause of the change within a cell is unknown. When a cell is mutated, it can also grow uncontrollably and destroy the healthy cells around them. Typically, NSCLC may have spread to other tissues outside of the lungs by the time the cancer is diagnosed.
Risk factors and symptoms
Although NSCLC can occur in people who have never smoked, people who smoke are at a greater risk of developing lung cancer. Additionally, exposure to second-hand smoke, age, pollutants, exposure to carcinogenic materials, previous lung diseases, and family history of lung cancer might contribute to the development of lung cancer. A chronic cough, chest pains, fatigue, trouble breathing and swallowing, wheezing, and hoarseness are some of the symptoms of NSCLC. Diagnosis of NSCLC is difficult due to many symptoms overlapping with other common diseases. Several clinical tests such as biopsies, sputum analysis, and imaging tests are used to detect NSCLC.
Treatment options
The majority of patients with NSCLC survive at least 5 years (https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics). However, if the cancer has spread to other tissues, the survival rate is much lower. In the past several years, a steady increase in research in the field has assisted in understanding NSCLC at a deeper level and resulted in the development of therapeutics, thereby offering more medical options for patients with NSCLC. Currently, the most common treatment options are surgery (if NSCLC is localized to the lung and has not spread), chemotherapy, radiation, targeted therapy, and immunotherapy. Immunotherapy is a breakthrough treatment that aims to alter the patient’s immune system to enable it to locate and eradicate cancer cells specifically.
We have discussed some specific aspects of immunotherapy previously on OncoBites. Therefore, in this article, we provide a general overview of how many immunotherapies work.
How does immunotherapy work?
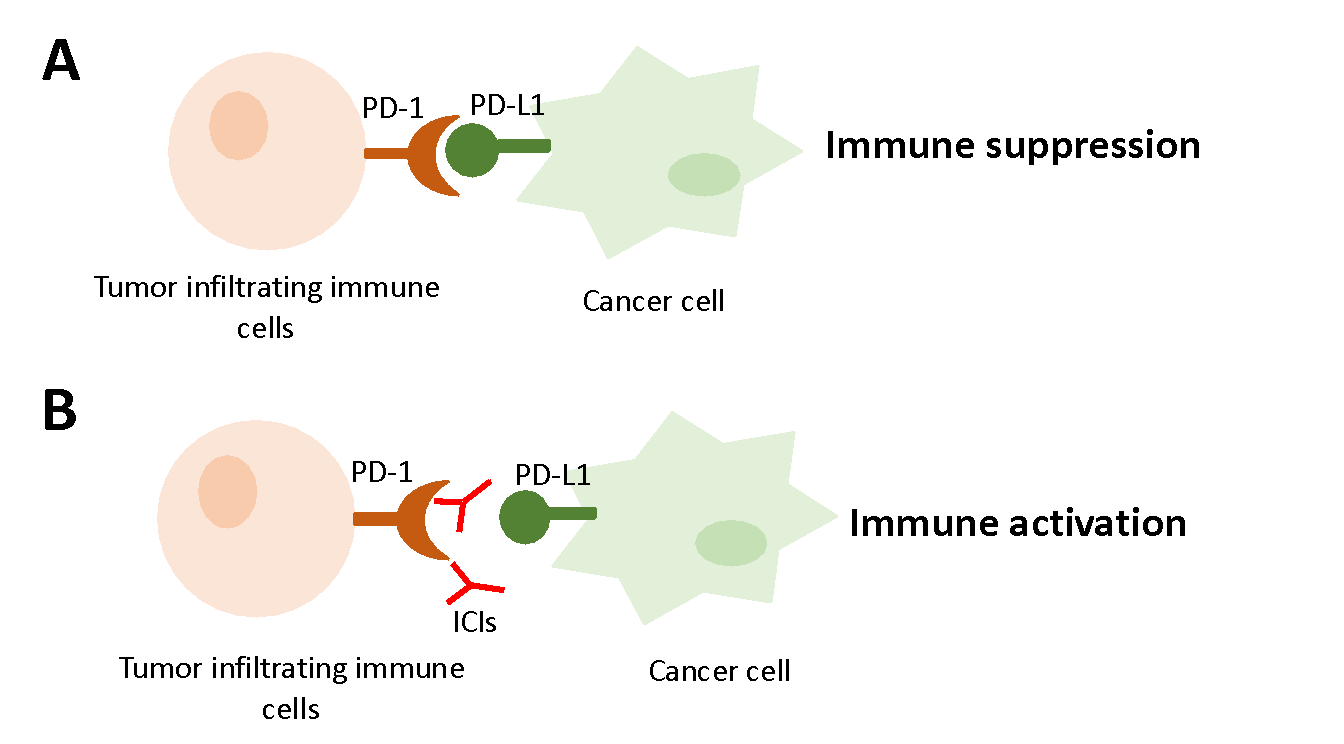
Recently, it was discovered that immune cells present at the tumor site can express a receptor called programmed death-1 (PD-1). A cell receptor is a protein on the cell membrane that can bind to a ligand (a molecule that binds to a receptor) on the outside surface of the cell. Receptor-ligand interaction can activate or inhibit a cell. PD-1 can bind to its ligand and affect the function of immune cells by initiating a brake-like mechanism (figure 1). Ligands for PD-1, called programmed death-ligand (PD-L1 and PD-L2), are expressed on tumor cells. When immune cells and cancer cells interface with each other, the interaction between PD-1 and PD-L1/PD-L2 helps cancer cells to escape from the immune system.
Seminal research works have led to the development of specific therapeutic products that can block the PD-1/PD-L1 interaction, releasing the brakes off of immune cells and thereby inducing tumor cell killing. These therapeutic products are commonly known as immune checkpoint inhibitors (ICIs). ICIs have changed the treatment strategy for many advanced-stage cancers, including NSCLC, and many studies have reported beneficial outcomes with these therapies compared to chemotherapy and improved overall survival significantly. Several immunotherapies have been approved for use, such as Opdivo (Nivolumab), Keytruda (Pembrolizumab), and Imfinzi (Durvalumab) to treat a variety of cancer types including NSCLC. Oncologists use biomarkers such as programmed death-1 (PD-L1) to determine whether chemotherapy or immunotherapy or a combination of the two might be a better treatment strategy for a cancer patient. Patients with high levels of PD-L1 expression is associated with better response to ICIs and have better clinical outcomes although some cancer types do not show an exact correlation between PD-L1 expression and the response to immunotherapies. Therefore, biomarker development is an important step in enhancing the therapeutic effects of ICIs. The science of immunotherapy is still progressing and is available to patients with certain cancers including NSCLC.
Edited by Prathyusha Konda
Research Works Referenced:
1. Grant MJ, Herbst RS, Goldberg SB. Selecting the optimal immunotherapy regimen in driver-negative metastatic NSCLC. Nat Rev Clin Oncol. 2021;18(10):625-44. Epub 2021/06/26. doi: 10.1038/s41571-021-00520-1. PubMed PMID: 34168333.
2. Doroshow DB, Bhalla S, Beasley MB, Sholl LM, Kerr KM, Gnjatic S, Wistuba II, Rimm DL, Tsao MS, Hirsch FR. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nature Reviews Clinical Oncology. 2021;18(6):345-62. doi: 10.1038/s41571-021-00473-5.
