Reading time: 4 minutes
Chris Wang
Unlike the Merriam Webster definition of promiscuous, describing a kinase inhibitor as promiscuous actually refers to the number of kinases it inhibits. The more promiscuous an inhibitor is, the higher number of off-targets it has. Traditional drug development strategies avoid promiscuous compounds because off-target effects can lead to side effects. For example, the reason why the antihistamine diphenhydramine makes people sleepier than the non-drowsy antihistamine cetirizine is because of off-target effects.
Kinase inhibitors are a class of drugs that have exploded in FDA approval indications in cancer since the first kinase inhibitor imatinib was approved in 2001. While imatinib was originally designed as an inhibitor of the BCR-ABL kinase for use in chronic myeloid leukemia (CML), the activity of imatinib on off-target kinases allows it to have multiple uses. In addition to treating CML, imatinib is used to treat a variety of rare cancers including a type of skin cancer (DFSP) and an uncommon form of cancer in the GI tract (GIST). This ability of imatinib to treat wide ranging cancer types is directly due to its multi-target inhibition of the C-KIT, PDGFR-alpha, and BCR-ABL kinases (Figure 1).

Imatinib was a drug designed for CML based on its ability to inhibit the BCR-ABL fusion kinase in drug screening. BCR is a tyrosine kinase that stimulates cell growth and is normally turned off with a self-regulatory domain. However, when fused to the ABL protein, the mutated BCR-ABL loses its ability to auto-regulate and instead is always on. This leads to the oncogenesis of CML cells. While imatinib was the first compound designed to inhibit BCR-ABL and treat CML, its ability to inhibit the off-target kinases C-kit and PDGFR was found less than a year after it was first studied in humans.
DFSP and GIST cancers utilize PDGFR and c-KIT kinases to grow uncontrollably. Similar to how CML cells BCR-ABL fusion protein, PDGFR is fused to a collagen protein within DFSP tumors. The protein then forms an uncontrollable signal to divide continuously. In contrast, over 80% of GIST tumors have activating point mutations in the c-KIT receptor tyrosine kinase that lead to constitutive activation even in the absence of its binding ligand. Because DFSP and GIST cells exploit these kinases to grow, imatinib has shown clinical benefit in both DFSP and GIST tumors that cannot be removed from surgery (unresectable) or that come back after initial surgery (relapsed).
With this information you might think it is a good idea to create a kinase inhibitor that inhibits every known kinase involved in cancer,allowing you to have a universal drug. However, a major drawback of this idea is that off-target kinase inhibition carries additional risks for side effects. One of the most common toxicities of imatinib use is edema, or fluid accumulation, and low blood cell counts, which is directly related to its off-target inhibition. While edema from imatinib mainly includes less dangerous swelling under the eyes (periorbital) or in the lower limbs, it can sometimes lead to severe fluid accumulation around the lungs and heart (pleural and pericardial effusion). Low blood counts include low platelets, white blood cells, and red blood cells which can range from mild to severe, some requiring blood transfusions.
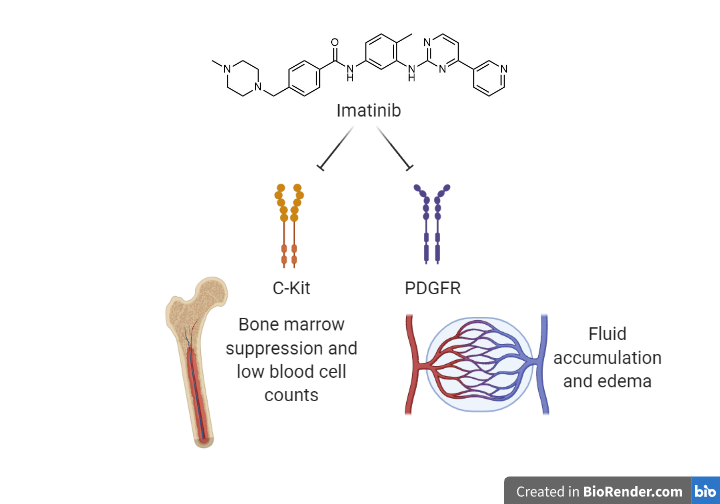
The molecular basis of these side effects can be traced back to the off-target inhibition of c-KIT and PDGFR (Figure 2). Since c-KIT is expressed in stem cells within the bone marrow that creates blood cells and platelets, inhibition by imatinib can result in low blood cell counts. Similarly, PDGFR plays a role in regulating interstitial fluid pressure (IFP) and upon inhibition causes the pressure to fall. This decrease in IFP allows hydrostatic pressure from blood vessels to push fluid out of capillaries, resulting in fluid accumulation outside of the blood. Thus, the benefit of imatinib’s off-target effects is also directly the reason for its side effects.
The ability of promiscuous multi-kinase inhibitors to have multiple uses is not limited to just imatinib. Many multi-kinase inhibitors such as sunitinib, sorafenib, and cabozantinib have been developed and are used in multiple solid and hematological malignancies. However, when developing a kinase inhibitor, researchers need to weigh the pros and cons of kinase selectivity (Figure 3). While multi-kinase kinase inhibitors have shown clinical uses in multiple types of cancer, the side effect profile may limit their use and more research is needed to expand the use of currently available promiscuous inhibitors.
Edited by MaryAnn Bowyer
Abbreviations: GIST, gastrointestinal stromal tumor; DFSP, dermatofibrosarcoma protuberans; BCR-ABL, breakpoint cluster region protein-tyrosine-protein kinase ABL1 fusion protein; c-KIT, proto-oncogene c-KIT; PDGFR, platelet-derived growth factor receptors.
References
Iqbal N, Iqbal N. Imatinib: A Breakthrough of Targeted Therapy in Cancer. Chemother Res Pract. 2014; 2014: 357027.
Giles FJ, O’Dwyer M , Swords R. Class effects of tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia. Leukemia. 2009 Oct;23(10):1698-707. doi: 10.1038/leu.
Pietras K, Sjöblom R, Rubin K, Heldin CH, Ostman A. PDGF receptors as cancer drug targets. Cancer Cell. 2003 May;3(5):439-43. doi: 10.1016/s1535-6108(03)00089-8.

Leave a comment