
Reading time: 6 minutes
Andrew C. Griggs, Jordan E. Rogers, Elizabeth H. Lazzara
Research Engineering and Applied Collaborations in Healthcare (REACH) Lab
Patients with cancer may be at greater risk of contracting or developing complications related to COVID-19. Given the lack of a vaccine or specific antiviral therapy for COVID-19 at this time, the large emphasis currently placed on infection prevention is appropriate. Cancer care involves the coordination of multiple healthcare professionals, thus increasing the opportunities for transmission. Multidisciplinary tele-teams are recommended to help clinically monitor and treat low-risk patients with cancer during the current pandemic. Communication tools used to disseminate information to patients and visitors are becoming increasingly necessary, and many treatment centers are now performing telemedical services for patients that may be exhibiting symptoms of COVID-19. Telemedicine, which Grundy et al. defined as “medicine practiced from a distance using telecommunications,” is often described as synchronous and asynchronous. In practice, synchronous (real-time) telemedicine refers to audiovisual interactions between patients and providers; meanwhile, asynchronous (non-real-time) applications include systems such as electronic health records or store-and-forward systems.
Telemedicine is now slated to become an extremely important tool for minimizing the impacts of the COVID-19. In addition to revisions in policy, such as the 2018 Bipartisan Budget Act or the 2019 Connected Care Pilot Program that have enabled greater utilization of telemedicine in the United States, the WHO is recommending the use of telemedicine for patient evaluations to reduce opportunities for infection. Moreover, regulations have been relaxed further in the United States to address COVID-19, as evidenced by multiple recent policy changes allowing for physicians to provide telemedicine services across state lines and provisions for improved reimbursement for providers (e.g. Centers for Medicare and Medicaid Services (CMS) Waiver 1135 & the Coronavirus Preparedness and Response Supplemental Appropriations Act). These policy changes are a pragmatic step forward, as telemedicine services can reduce opportunities for infection for patients and providers alike during the current COVID-19 pandemic. In fact, some are calling for cancer centers to increase the integration of telemedicine even more to alleviate some of the obstacles imposed by COVID-19. However, telemedicine may be inherently limited by patients’ access to the internet and proficiency in technology. Telemedicine may not be as advantageous for impoverished cancer patients without access to resources such as smartphones, computers, or reliable internet access. Similarly, factors such as age and educational achievement can influence cancer patients’ willingness to utilize certain applications of telemedicine, such that college-educated younger adults exhibit the greatest amount of willingness.
The application of telemedicine to advance cancer care is referred to as teleoncology. Given the complexity of cancer care, there are still multiple oncological functions that can be performed within the context of telemedicine. Teleoncology offers numerous benefits for cancer patients. Teleoncology can be used to support lifestyle modification, wellness activities, and medication adherence. Teleoncology can be used to help facilitate the connections between the patient and their care team to provide coaching and feedback to support lifestyle modification. In addition, teleoncology can promote wellness activities such as exercise and meditation. Further, teleoncology can support medication adherence by facilitating reminders. Figure 1 provides a graphical representation of some of the types of telemedicine used within teleoncology.
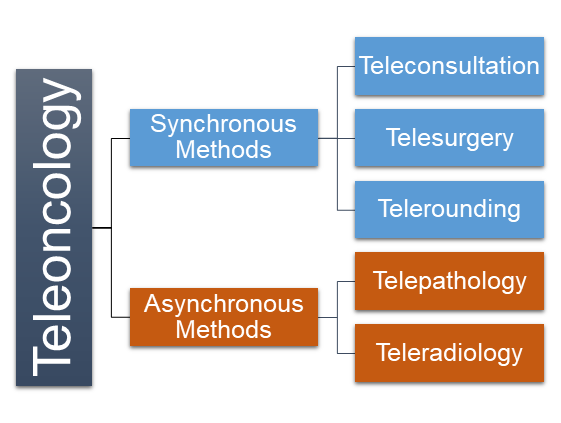
Synchronous Methods
Teleconsultation and videoconferencing involve patient-caregiver communications that occur via email, phone, automated messaging systems, or real-time face-to-face contact via videoconferencing equipment. Both teleconsultation and videoconferencing can act as proxies for in-person visits and, therefore, serve to streamline care by eliminating the time and costs associated with traveling to healthcare facilities. In addition, teleconsultation and videoconferencing are beneficial for rural patient populations, as they improve patients’ access to specialist consultations. The benefits of teleconsultation and videoconferencing should be weighed against potential technological difficulties, however, and communication challenges may arise due to the lack of face-to-face contact. Because of this, it is suggested that conversations involving sensitive details (e.g., providing a diagnosis or prognosis) be held in person. Telesurgery is also known as robotic surgery and involves operating on a patient from a remote location. Traditionally, surgeons interact directly with the patient anatomy while standing at the operating room table to perform the operation. In contrast, surgeons performing robotic surgery are seated within a console and remotely control the surgical instruments working on the patient. Telesurgery is best when used on minimally-invasive surgeries and offers several clinical advantages (e.g., decreased blood loss, smaller incision sites, and shorter recovery times) that may be especially beneficial for cancer patients. Telerounding replaces the rounds that clinical staff typically perform (e.g. checking on patients) using remote-controlled mobile technology maneuvering on the patient floor to facilitate diagnosis, patient care, and management. The mobile technology “visits” the patient’s bedside and typically transmits video and auditory data in real time to one or more providers in a remote location. Given that patients with cancer often have suppressed immune systems, it is advantageous to reduce patients’ exposure to unnecessary pathogens. Consequently, telerounding may be a highly useful option when multiple providers are needed to discuss care plans.
Asynchronous Methods
Telepathology and teleradiology involve the transfer of image-rich pathology data and radiological images (e.g., X-rays, CTs, and MRIs), respectively, from one location to another to share with other clinicians to support diagnosis, education, and research. Both of these approaches to sharing clinical data are advantageous applications of telemedicine whereby multidisciplinary and interprofessional teamwork can be supported regardless of distance and travel restrictions due to Coronavirus.
Conclusion
Patients with cancer are at a greater risk of developing complications related to COVID-19. Oncology providers around the world therefore have an obligation to explore applications such as telemedicine to protect their employees and patients alike from unnecessary risks during the current pandemic. There are many considerations that must accompany the decision to utilize telemedicine, as many factors can influence patients’ access and willingness to use such services. Telemedicine may not be as useful for highly dynamic cancer cases, for patients with limited access to the internet, or for patients with low familiarity with technology. Additionally, synchronous applications of telemedicine requiring robotic systems, such as some forms of telerounding and telesurgery, will require training for providers to ensure effective implementation.
Regardless, telemedicine is anticipated to be an invaluable tool in oncology during the COVID-19 pandemic. Regulations and policies have been relaxed in response to COVID-19 to catalyze the use of telemedicine in the United States and to ensure improved reimbursement for providers. Every application previously discussed is an effective avenue to reduce opportunities for infection without compromising the quality of care received by patients. These applications can be leveraged individually, in conjunction with each other, or in conjunction with traditional face-to-face avenues to provide care for cancer patients. Asynchronous applications of telemedicine are already commonplace in many practices, such as the use of digital healthcare records, but they can be further leveraged to supplement synchronous applications by transmitting a greater amount of patient information digitally rather than face-to-face. This, in turn, can reduce the strain currently placed on PPE supplies by reducing the amount of face-to-face interactions involved in providing care. Telemedicine can also reduce the costs for patients associated with receiving care by reducing the amount of time and travel required to receive care in-person. Inevitably, not all patients or providers will be able to transition to digital modalities exclusively, however, a significant portion of clinical functions within oncology can be effectively delivered through telemedicine applications with realized benefits for patients and providers.
Edited by Sara Musetti
References
Alhalabi, O., & Subbiah, V. (2020). Managing cancer care during the COVID-19 pandemic and beyond. Trends in Cancer. https://doi.org/10.1016/j.trecan.2020.04.005
American Telemedicine Association. (2020). Telehealth basics. American Telemedicine Association. https://www.americantelemed.org/resource/why-telemedicine/
Bogen, E. M., Aarsæther, E., Augestad, K. M., Lindsetmo, R. O., & Patel, H. R. (2013). Telemedical technologies in urological cancer care: Past, present and future applications. Expert Review of Anticancer Therapy, 13(7), 795-809.
Boscoe, F. P., Henry, K. A., Sherman, R. L., & Johnson, C. J. (2016). The relationship between cancer incidence, stage and poverty in the United States. International Journal of Cancer, 139(3), 607-612.
Choi, P., Oskouian, R., & Tubbs, R. (2018). Telesurgery: Past, present, and future. Cureus, 10(5). https://doi.org/10.7759/cureus.2716
Cinar, P., Kubal, T., Freifeld, A., Mishra, A., Shulman, L., Bachman, J., Fonseca, R., Uronis, H., Klemanski, D., Slusser, K., Lunning, M., & Liu, C. (2020). Safety at the time of the COVID-19 pandemic: How to keep our oncology patients and healthcare workers safe. Journal of the National Comprehensive Cancer Network, 18(5), 1-6. https://doi.org/10.6004/jnccn.2020.7572
Contreras, C. M., Metzger, G. A., Beane, J. D., Dedhia, P. H., Ejaz, A., & Pawlik, T. M. (2020). Telemedicine: Patient-provider clinical engagement during the COVID-19 pandemic and beyond. Journal of Gastrointestinal Surgery. https://doi.org/10.1007/s11605-020-04623-5
Daly, B., Baldwin-Medsker, A., & Perchick, W. (2019, November). Using remote monitoring to reduce hospital visits for cancer patients. Harvard Business Review. https://hbr.org/2019/11/using-remote-monitoring-to-reduce-hospital-visits-for-cancer-patients
Doarn, C. R., Pruitt, S., Jacobs, J., Harris, Y., Bott, D. M., Riley, W., Lamer, C., & Oliver, A. L. (2014). Federal efforts to define and advance telehealth—A work in progress. Telemedicine and e-Health, 20(5), 409-418. https://dx.doi.org/10.1089%2Ftmj.2013.0336
Grundy, B. L., Crawford, P., Jones, P. K., Kiley, M. L., Reisman, A., Pao, Y. H., Wilkerson, E. L., & Gravenstein, J. S. (1977). Telemedicine in critical care: An experiment in health care delivery. Journal of the American College of Emergency Physicians, 6(10), 439-444. https://doi.org/10.1016/S0361-1124(77)80239-6
Guthrie, G. (2018, October 23). How teleoncology helps deliver high-quality cancer care. Cancer.net. https://www.cancer.net/blog/2018-10/how-teleoncology-helps-deliver-high-quality-cancer-care
Harky, A., Chiu, C. M., Yau, T. H. L., & Lai, S. H. D. (2020). Cancer patient care during COVID-19. Cancer Cell. Advance online publication.
Hazin, R., & Aaddoumi, I. (2010). Teleoncology: Current and future applications for improving cancer care globally. Lancet Oncology, 11(2), 204-210.
Liang, W., Guan, W., Chen, R., Wang, W., Li, J., Xu, K., Li, C., Ai, Q., Lu, W., Liang, H., Li, S., & He, J. (2020). Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. The Lancet Oncology, 21(3), 335-337. https://doi.org/10.1016/S1470-2045(20)30096-6
Marescaux, J., Leroy, J., Gagner, M., Rubino, F., Mutter, D., Vix, M., Butner, S. E., & Smith, M. K. (2001). Transatlantic robot-assisted telesurgery. Nature, 413(6854), 379-380.
Okereafor, K., Adebola, O., & Djehaiche, R. (2020). Exploring the potentials of telemedicine and other non-contact electronic health technologies in controlling the spread of the novel coronavirus disease (COVID-19). International Journal in IT & Engineering, 8(4). 1-13.
Okuyama, S., Jones, W., Ricklefs, C., & Tran, Z. V. (2015). Psychosocial telephone interventions for patients with cancer and survivors: A systematic review. Psycho‐Oncology, 24(8), 857-870.
Potdar, R., Thomas, A., DiMeglio, M., Mohiuddin, K., Djibo, D. A., Laudanski, K., Dourado, C. M., Leighton, J. C., & Ford, J. G. (2020). Access to internet, smartphone usage, and acceptability of mobile health technology among cancer patients. Supportive Care in Cancer, 1-7.
Sabesan, S., Larkins, S., Evans, R., Varma, S., Andrews, A., Beuttner, P., Brennan, S., & Young, M. (2012). Telemedicine for rural cancer care in North Queensland: Bringing cancer care home. Australian Journal of Rural Health, 20(5), 259-264. doi.org/10.1111/j.1440-1584.2012.01299.x
Satcher, R., Bogler, O., Hyle, L., Lee, A., Simmons, A., Williams, R., Hawk, E., Matin, S., & Brewster, A. (2014). Telemedicine and telesurgery in cancer care: Inaugural conference at MD Anderson Cancer Center. Journal of Surgical Oncology, 110(4), 353-359.
Schapira, L. (2019, March 20). Telemedicine in cancer care: Rewards and risks. Cancer.net. https://www.cancer.net/blog/2019-03/telemedicine-cancer-care-rewards-and-risks
Sirintrapun, J., & Lopez, A. M. (2018). Telemedicine in cancer care. American Society of Clinical Oncology Educational Book, 38, 540-545.
Ueda, M., Martins, R., Hendrie, P. C., McDonnell, T., Crews, J. R., Wong, T. L., McCreery, B., Jagels, B., Crane, A., Byrd, D. R., Pergam, S. A., Davidson, N. E., Liu, C., Stewart, F. M. (2020). Managing cancer care during the COVID-19 pandemic: Agility and collaboration toward a common goal. Journal of the National Comprehensive Cancer Network, 18(4), 366-369. https://doi.org/10.6004/jnccn.2020.7560
Verhoeven, F., van Gemert-Pijnen, L., Dijkstra, K., Nigland, N., Seydel, E., & Steehouder, M. (2007). The contribution of teleconsultation and videoconferencing to diabetes care: A systematic literature review. Journal of Medical Internet Research, 9(5). https://doi.org/10.2196/jmir.9.5.e37
World Health Organization. (2020, March 19). Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): Interim guidance, 19 March 2020 (World Health Organization Publication No. WHO/2019-nCoV/IPC PPE_use/2020.2). World Health Organization. https://reliefweb.int/report/world/rational-use-personal-protective-equipment-ppe-coronavirus-disease-covid-19-interim
World Health Organization. (n.d.). eHealth. who.int. https://www.who.int/ehealth/en/
Image Credits
https://pixabay.com/illustrations/doctor-online-medical-chat-4068134/
