
Reading time: 6 minutes
Manisit Das
Sometimes double agents can be critical players in changing the course of conflicts, wars, and history. If you are a Potterhead like me, you are probably aware of how Professor Severus Snape played an important role in the wizarding world of Harry Potter. He instigated many of the major events in the story, and was finally revealed to be working as a double agent all along much to the surprise of the readers!
Today we will be talking about ‘cellular double agents’ that were recruited to fight cancer. Engineered cells are not a new player in cancer therapy. At Oncobites, we previously discussed CAR-T cells, an immune cell-based anticancer therapy. In this therapeutic approach, the patient’s own immune cells are isolated from their blood, and after engineering the immune cells to target cancer, they are returned back to the patient. The first CAR-T based therapy was approved for patient use last year. The approval came for Acute Myeloid leukemia, a cancer of the white blood cells, after the therapy achieved remission, a period where the signs and symptoms of cancer disappear, in 52 out of 63 patients. While only about 4 to 5 out of 10 patients will live up to the one year mark with this disease, the response seen was encouraging, warranting the approval of the drug. Recently, CAR-T therapies were also been approved for some types of lymphomas which are cancers of a part of the immune system called lymph. As cell-based therapies are rapidly moving in the clinic, researchers are exploring what kind of cells can be used for therapeutic purposes. Some are wondering if we can potentially engineer cancer cells to fight against other cancer cells? A recent study conducted by researchers at Harvard Medical School shows that it is possible, at least in mice.
The study was determined to answer two main questions:
- Can we isolate the patient’s own cells and engineer them for therapeutic purposes? Using our own cells is beneficial, as our immune system is extremely sensitive to foreign cells as part of our natural defense mechanisms. However, that also creates problems sometimes. You may have heard that finding a suitable match during organ transplantations can be difficult, and more than often, organs are rejected by the patient’s body leading to failure of the therapy. Using our own cells is beneficial, as our immune system will not actively trying to fight the engineered cells, allowing the cells to survive within our body for a long time performing their duties.
- Can we kill off the cancer cells once they finish their job? At the end of the day, these cancer cells used for therapy are still abnormal cancer cells with a potential to develop tumors. To ensure that the therapy is safe and that they do not survive only to be Frankenstein: the monster you created, you need to equip the cells with a switch that you can use to trigger their death after the cancer cells that you intended to kill are gone.
To help the cancer cells satisfy their pursuit, the study looked at a molecule called TRAIL. This protein molecule is known to induce cell death after binding to other proteins expressed on the cell surface called….(drum roll!) death receptors. The cancer cells were isolated from tumors growing in mice and were engineered out of the body to secrete TRAIL into the surrounding environment of the cells. The idea was that the cancer cells will home to the tumor and secrete TRAIL molecules which can go on to bind with death receptors on the cancer cells causing them to die.
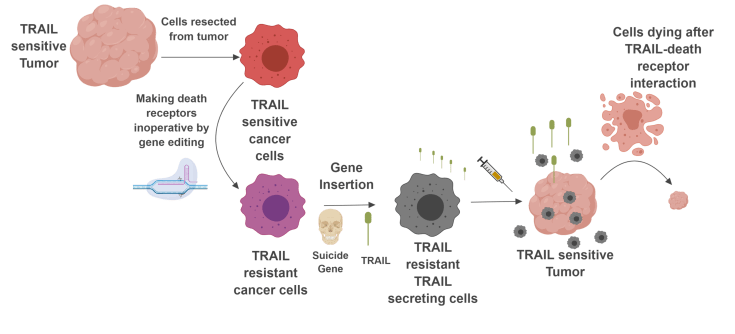
There is, however, a small problem with this idea. The cancer cells that are serving as little TRAIL factories are not protected from the effect of death receptor interaction with TRAIL themselves. To protect these therapeutic cells, the researchers made the death receptor genes on these cells inoperative, allowing them to survive after binding with TRAIL. Now you got cells that can secrete the therapeutic protein, and at the same time resistant to the protein’s effect, letting them do their business. The final piece of the problem was to introduce a mechanism to kill the cells after they perform their duty. This was done by inserting a ‘suicide gene’.
A suicide gene, when introduced in a cell, make it produce special enzymes. These enzymes modify certain drugs in a specific way such that the changed molecule will behave as a lethal agent to the cell. This eventually allows the administration of the drug to kill a specific population of cells when intended. The same strategy had been used in the past to develop antiviral drugs, taking advantage of how viral enzymes can process certain molecules, producing toxic substances. This current study introduces a similar viral enzyme to the cancer cells, allowing them to replicate the function of the virus, providing the researchers with the capability to trigger a targeted killing of engineered cells by administering the antiviral drug.
In this work, the scientists tested this strategy in a mouse model of glioblastoma, an aggressive cancer of the brain. They found that the mouse-derived brain cancer calls after engineering are resistant to the effects of TRAIL, and after injecting back to the animal, the cells can be killed off with the antiviral drug. Once it was made sure that this strategy works, they exploited the engineered cancer cells as a therapy against the original tumor from which the therapeutic cancer cells were developed. They found that the engineered cancer cells were successful in shrinking the original tumor, and they could further be killed off by the antiviral drug, showing that this approach works.
So what does all of these mean? The cell engineering approach was a unique strategy using the cancer cells against the cancer cells. Nevertheless, there are several challenges associated with translating this approach into a clinical option. The therapy worked very well when the engineered cancer cells were introduced very close to the actual tumor, however, when it was administered in a remote location, the therapy didn’t work so well. This may be a challenge with human tumors, where tumor nodules that are inaccessible to the therapy may eventually result in the relapse of the disease. Secondly, time is a crucial factor in cancer therapy. Collecting cells from a patient, and engineering them, and doing all the safety check before putting back to the patient takes a lot of time, which may not always be available with cancer. Finally, these complex engineering processes can get really expensive. The recently approved CAR-T therapy comes with a hefty price tag of $475,000. This is just the cost of the procedure, not inclusive of other expenses like hospital stay and visits to the physicians. That being said, gene therapy is rapidly making progress. From worms to cures, it took us about two decades to get the world’s first RNA interference-based gene silencing drug. The first study on CAR-T cells was published in 1989. We had to wait until 2017 to get a clinically approved therapy. So we do have a long way to go. Using the insights gathered from clinical development and preclinical research, we can be optimistic about reducing the timeline required to engineer the cells and reducing its expenses.
In the Harry Potter series, Professor Snape played a crucial role in bringing the downfall of Lord Voldemort while working from the dark side within, and sacrificing his life in the process. These engineered cancer cells are an army of Snapes to our immune system. However, as we discussed, cancer is inherently complex and this therapeutic approach has its challenges. To our non-magical people, whether cellular double agents will be a significant clinical approach, time will tell.
Work Discussed
Reinshagen, C., Bhere, D., Choi, S. H., Hutten, S., Nesterenko, I., Wakimoto, H., . . . Shah, K. (2018). CRISPR-enhanced engineering of therapy-sensitive cancer cells for self-targeting of primary and metastatic tumors. Sci Transl Med, 10(449). doi: 10.1126/scitranslmed.aao3240
Image Credits
Severus Snape: Sonserina

Leave a comment