Reading time: 4 minutes
Mallory Kane
The immune system is the first line of defense in detecting and destroying cancer cells. Several mechanisms are in place to prevent and slow cancer growth. However, cancerous cells often can avoid destruction by the immune system. These cells may contain genetic mutations that make them invisible to immune cells, proteins that inactivate the immune system, or the inability to perform apoptosis.
Immunotherapy is an umbrella term for types of cancer treatments that engineer the body’s own immune cells to identify and destroy cancerous cells. There are several types of immunotherapies. Immune checkpoint inhibitors like Nivolumab and Ipilimumab inhibit the body’s ability to shut off the immune response, resulting in the immune cells’ overactivation. The result is a more robust immune response. Monoclonal antibodies like Trastuzumab and Cetuximab are synthetic antibodies programmed to mark cancer cells for destruction by immune cells. Immune system modulators like Imiquimod and Thalidomide cause increased release of cytokines and interferons, facilitating attack of cancerous cells. Treatment vaccines are another type of immunotherapy. These work by exposing the immune system to certain cancer proteins to recognize and kill cancer cells circulating in the body unnoticed.
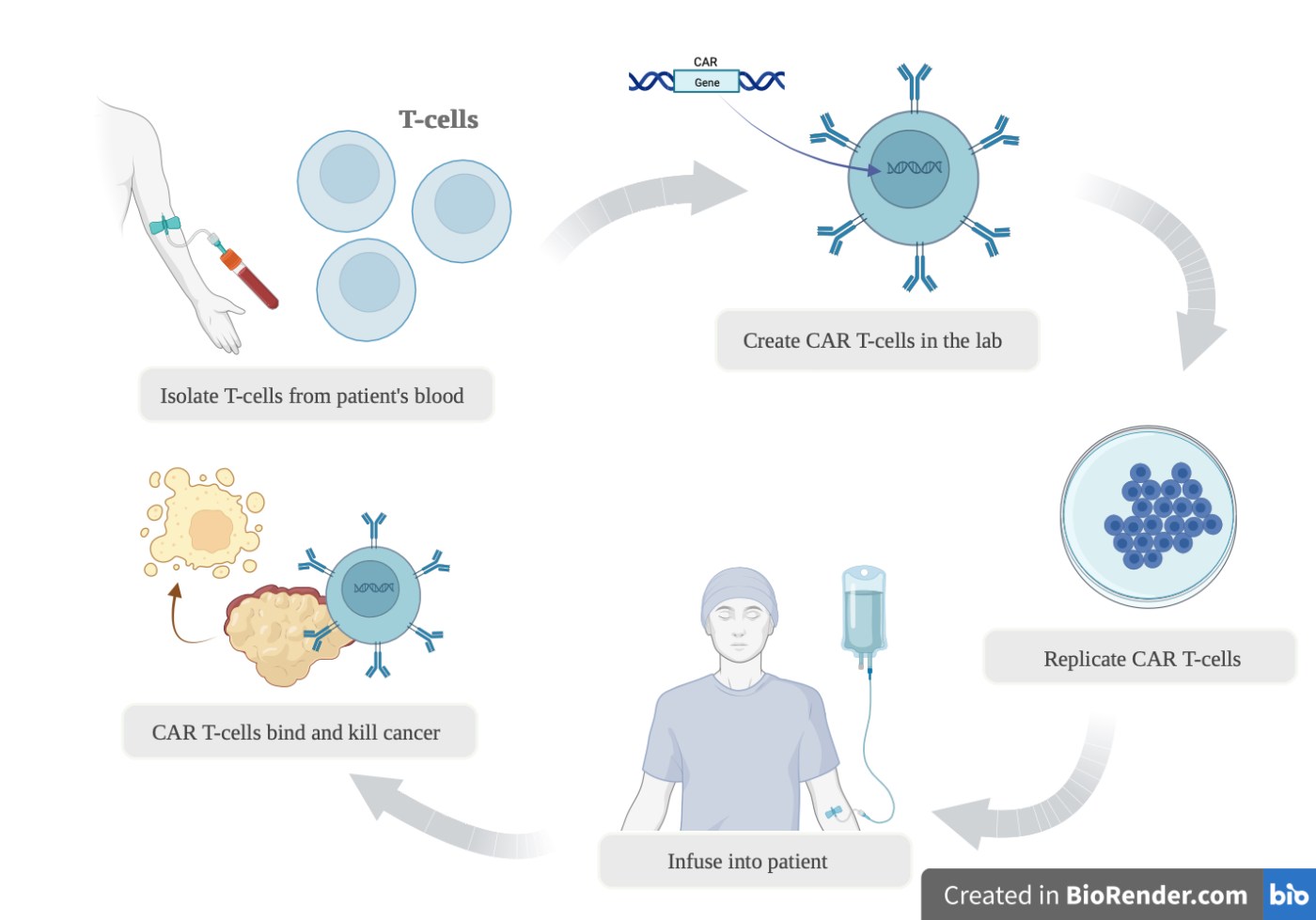
CAR-T cell therapy is a newer form of immunotherapy that amplifies the ability of T-cells to identify and kill cancer cells. Performing CAR-T cell therapy involves a personalized approach in which the patient’s immune cells are altered in a lab. Blood is removed from the patient, and T-cells are isolated. These cells are then synthetically altered to produce a protein called chimeric antigen receptor or “CAR,” which helps T cells recognize and attack cancer cells. CAR-producing T-cells are incubated until millions are produced. This can take approximately 3-8 weeks, during which the patient often receives chemotherapy to clear existing immune cells, allowing CAR-T cells to work better. Once enough CAR-T cells are produced, they are infused into the patient.
CAR-T cell therapies have several side effects which limit their use. This includes cytokine release syndrome (CRS), tumor lysis syndrome, graft versus host disease, and immune effector cell-associated neurotoxicity syndrome. All these adverse effects can cause lasting damage to the body or be fatal. CRS is the most common, with some trials suggesting that up to 75% of patients get CRS after CAR-T cell infusion, and almost half of these patients get admitted to the intensive care unit (ICU). The risk of these side effects can persist beyond the initial infusion while CAR-T cells remain in the blood. Long-term follow-up in B-cell lymphoma patients has found CAR-T cells in the blood over 10 years after infusing them. Researchers are trying to develop a way to eliminate CAR-T cells from the body once the anti-cancer response is achieved to mitigate the risk of long-term side effects. Some studies have attempted to use biodegradable CAR-T cells, which could hold promise. However, there is concern that eliminating CAR-T cells after they take effect could cause cancer relapse.
Another important limiting factor in the use of CAR-T cell therapy is cost. Its high price of approximately $400,000 per infusion is a barrier to many patients receiving this treatment. A more cost-effective method for completing this therapy needs to be discovered.
CAR-T cell therapy holds promise for treating lymphomas and leukemias, with six different therapies approved by the US Food & Drug Administration (FDA) since 2017. However, this therapy is currently only FDA-approved for hematologic malignancies and is not used to treat solid tumors. Recent discoveries suggest that CAR-T cell therapy could hold promise for certain solid malignancies. Ongoing clinical trials are investigating the use of CAR-T cell exchange for triple-negative breast cancer, metastatic prostate cancer, adenocarcinoma of the pancreas, malignant brain gliomas, and anaplastic and medullary thyroid cancer.
Immunotherapy’s CAR-T cell transfer is on the rise. New advances are required to decrease the adverse effects of this treatment and lower its cost, but with upcoming studies expanding its use to solid tumors, this treatment could be a large step forward in the world of oncology.
Edited by Pratyusha Ghanta
References:
Choi G, Shin G, Bae S. Price and Prejudice? The Value of Chimeric Antigen Receptor (CAR) T-Cell Therapy. Int J Environ Res Public Health. 2022;19(19):12366. Published 2022 Sep 28. https://doi:10.3390/ijerph191912366
Enfu Hui; Immune checkpoint inhibitors. J Cell Biol 4 March 2019; 218 (3): 740–741. doi: https://doi.org/10.1083/jcb.201810035
Manasi, J.P., Lakshmi, R.R., Fatima, K. et al. CAR T-Cell-Based gene therapy for cancers: new perspectives, challenges, and clinical developments. Frontiers in Immunology. 13 (2022). https://doi.org/10.3389/fimmu.2022.925985
Melenhorst, J.J., Chen, G.M., Wang, M. et al. Decade-long leukaemia remissions with persistence of CD4+ CAR T cells. Nature 602, 503–509 (2022). https://doi.org/10.1038/s41586-021-04390-6
Saxena, M., van der Burg, S.H., Melief, C.J.M. et al. Therapeutic cancer vaccines. Nat Rev Cancer 21, 360–378 (2021). https://doi.org/10.1038/s41568-021-00346-0
Sterner, R.C., Sterner, R.M. CAR-T cell therapy: current limitations and potential strategies. Blood Cancer J. 11, 69 (2021). https://doi.org/10.1038/s41408-021-00459-7
Zahavi D, Weiner L. Monoclonal Antibodies in Cancer Therapy. Antibodies (Basel). 2020;9(3):34. Published 2020 Jul 20. https://doi:10.3390/antib9030034
