Reading time: 4 minutes
Aileen I Fernandez
When a foreign substance such as a cancer cell presents itself in the human body, it is able to communicate with cells of the human immune system. The cancer cell signals the immune system, telling it “Hey! Pump the brakes!”, thus instructing the immune system to not kill the cancer. Immunotherapy, a form of cancer treatment that can harness the ability of our powerful immune system, is used to combat this. One type of immunotherapy is known as immune checkpoint inhibitor therapies (ICIs). ICIs function by releasing these natural brakes of the human immune system: they tell our immune system ‘Hey! It’s ok, this cancer thing is BAD’ and block any communication from tumor cells. By stopping the message from passing to the immune cell, it can act accordingly and kill the foreign tumor cell.
ICIs are used as drug targets in multiple kinds of cancer including late-stage melanoma and lung cancer. While their benefits – measured by response to therapy (is the cancer shrinking?) or survival (are patients with cancer surviving longer?) – can be remarkable, some patients who receive ICIs do not respond at all to this kind of therapy. Additionally, studies by Chae, et al and Kim, et al, amongst others, have shown that in patients not selected to receive this kind of therapy, a portion of them would in fact benefit from receiving this treatment.
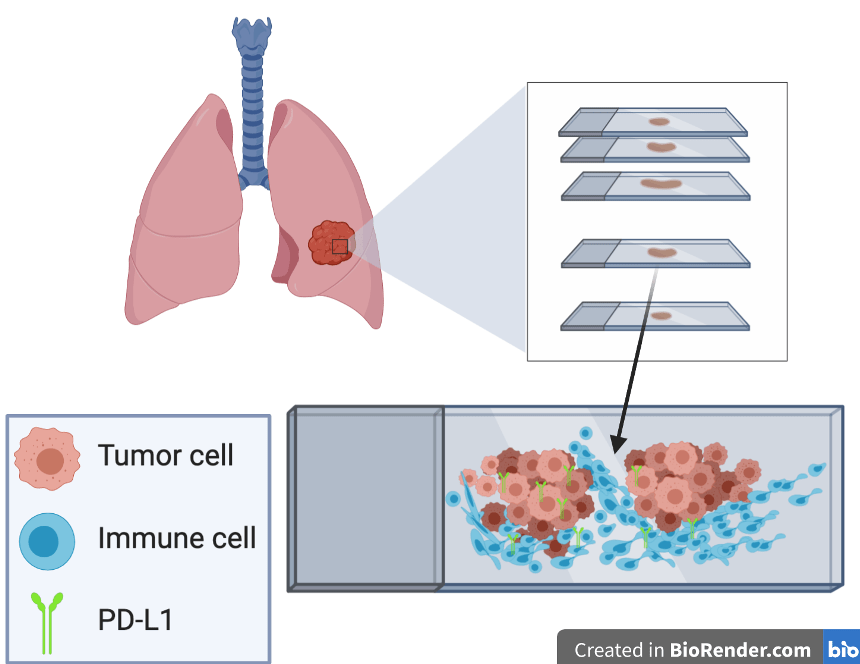
Currently in the clinical setting, we look at a tumor and decide which patient is going to receive ICIs by measuring the amount of a specific protein, PD-L1. This is the only FDA-approved companion diagnostic test for 4 different ICIs: pembrolizumab, nivolumab, atezolizumab, and durvalumab. However, we know that just looking at the expression of PD-L1 is not sufficient for determining what patients to treat. This is in part due to the fact that this protein is also expressed in immune cells and NOT only in cancer cells, which can obscure the interpretation (as shown in the above picture).
This leaves the need to find improved ways of identifying which patients will respond. Scientists have been working on several methods for improving this patient selection.
One method is using molecular prediction. For example, The Center for Cancer Research (CCR) in 2019 developed a new computational method that predicts which patient will respond to ICIs. The Ruppin lab used a 7187-patient sample set of 21 different cancer types. They tested their gene set in a validation cohort of roughly 300 melanoma patient samples and predicted almost all the ICI responders correctly.
Another promising method involves looking at additional proteins and their potential to be used in conjunction with PD-L1 as a predictor of response. Here we will discuss two: mismatch repair and tumor mutational burden.
The term mismatch repair (MMR) refers to “certain genes that are involved in correcting mistakes made when DNA is copied in a cell”. These are extremely vital in making sure that every time a new cell is made, any copy-and-paste errors are caught and fixed. Some tumors do not have their MMR machinery fully intact and so are considered “MMR deficient”; studies have shown that these tumors are more likely to respond to ICI treatment. Other studies have shown an association between MMR deficiency and an increased amount of PD-L1 protein. The culmination of this research has led to the approval of MMR deficiency as a biomarker of response to ICIs in metastatic cancers.
Tumor mutational burden (TMB) refers to how many mutations, or changes to the DNA, are present in cells (specifically cell types that are not passed down to children). Studies show that in certain tumor types, high TMB is associated with better response to ICIs and longer survival without disease worsening. However, there are challenges faced for using TMB in the clinic. These include deciding the minimum amount of mutations required to indicate if the patient with cancer should be given an ICI treatment, as well as finding a consistent and economical way of detecting TMB.
Overall, the discovery of ICIs has been groundbreaking in cancer treatment. However, there is a need to better decide which patients will receive which kind of immunotherapy. To date, the only diagnostic test we are using is PD-L1 expression, which has not reached the full potential of correctly predicting tumor response. There are many additional methods (molecular prediction, MMR deficiency, TMB) which in combination with PD-L1 can lead to improving patient care.
Edited by MaryAnn Bowyer
Works Discussed
Akinleye, Akintunde, and Zoaib Rasool. “Immune checkpoint inhibitors of PD-L1 as cancer therapeutics.” Journal of hematology & oncology 12.1 (2019): 92.
Carbone, David P., et al. “First-line nivolumab in stage IV or recurrent non–small-cell lung cancer.” New England Journal of Medicine 376.25 (2017): 2415-2426.
Davis, Andrew A., and Vaibhav G. Patel. “The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors.” Journal for immunotherapy of cancer 7.1 (2019): 278.
Jørgensen, Jan Trøst, and Karsten Bork Nielsen. “Companion and complementary diagnostics for first-line immune checkpoint inhibitor treatment in non-small cell lung cancer.” Translational Lung Cancer Research 7.Suppl 2 (2018): S95.

Leave a comment