
Reading time: 4 minutes
Michael Marand
In my last article, A Profile of Electric Fields in Cancer Therapeutics, I discussed Optune System, an electric field therapy for glioblastoma that disrupts cancer cell division and results in extended patient survival. I also presented an overview of some other potential applications of electric fields in cancer therapeutics, such as enhancement of radiation therapy, chemotherapy, and cell therapy. The focus of this installment is another electric-field-based cancer therapy called irreversible electroporation (IRE).
Since the 1950s, it has been shown that pulsed electric current can cause structural defects to the cell membrane. This knowledge has been employed in cancer therapeutics by aiding in the delivery of drugs (electrochemotherapy) and genetic material (electrogenetherapy). I would consider these methods to be the “Trojan Horse strategy”, in which a therapeutic agent infiltrates and causes cell death from within. IRE is more like artillery fire in that it damages the cells from the outside. IRE utilizes a series of short bursts of electric current to damage the membrane of diseased cells beyond the level of repair, ultimately leading to cell death in 6 to 48 hours.
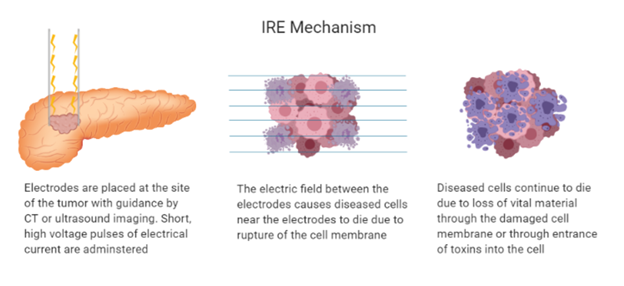
IRE is administered using between two and six electrodes, which are placed around a tumor. High voltage pulses are delivered through two probes at a time. No surgical incision is needed, and ultrasound or CT imaging is used to ensure probes are placed precisely around the tumor. The electrical pulses cause nanoscale pores to develop in the cell membrane of the diseased cells. The cells are killed by one of two mechanisms. The first mechanism occurs quickly as the voltage causes the cellular membrane that holds the cells together to be destroyed. This is more likely to happen to cells in close proximity to the probes. Alternatively, cells may retain pores for an extended period of time and die as a result of losing fluids, energy providing molecules, or vital organelles. These cells may also die due to uptake of toxic materials from outside the cell.
While the administration of high voltage may seem to be a safety concern, the current is only applied for short durations, which decreases its toxicity effects. Additionally, careful placement of the probes allows for cancerous cells to be killed without harming healthy tissue. Even if healthy cells are killed by the treatment, IRE does not disrupt the extracellular matrix, which is responsible for the structural support of the cells. This means that new cells can repopulate in place of the lost ones.
It is worthwhile to compare IRE to other, pre-existing methods of removing undesirable tissue. For example, thermal therapies such as radiofrequency (RF) heating or cryosurgery employ extreme heat and cold, respectively, to kill the cancer cells. However, these treatments each have disadvantages. In RF, the heat is dissipated by blood circulation resulting in unwanted heat to non-target areas. This would be like turning on the heat and leaving your front door wide open on a winter day. Likewise, blood circulation limits the success of cryotherapy by bringing unwanted heat to the target area. This would be like turning the A/C on and leaving your front door wide open on a summer day. Unlike RF and cryotherapy, IRE is able to overcome this heat transfer problem and is also faster to administer than thermal therapies. In addition to the inefficiencies mentioned above, thermal therapies also cause damage to off-target cells. IRE limits this as electroporated cells are able to conduct current better than cells outside of the treatment area demarcated with the probes.
The company Angiodynamics has been marketing a system for IRE therapy under the name NanoKnife since 2007, and the system has been used in over 5,400 procedures. Pulses are delivered in 10-30 minutes, but the entire surgery lasts 2-6 hours, depending on if other procedures are combined with IRE. In April of this year, Angiodynamics received approval from the FDA for clinical study of the treatment of stage III pancreatic cancer.
Research on potential applications of IRE are ongoing. For example, researchers at Virginia Tech have done preclinical work in dogs for the treatment of brain cancer with IRE, and since 2010, clinical trials for indications outside the brain have been going on worldwide. In 2013, a group in Australia demonstrated complete tumor destruction in thirteen out of eighteen patients. IRE has also been investigated clinically for prostate cancer and pancreatic cancer.
Research groups have been clear that IRE is not intended to be a first line therapy. However, IRE appears to be a promising therapeutic technique. In cases where radiation is not an option, such as in a case where a tumor is located near major blood vessels, IRE could be a very valuable alternative option.
Edited by Bekah Schulz
Works Discussed:
C. Jiang, R. V. Davalos and J. C. Bischof, “A Review of Basic to Clinical Studies of Irreversible Electroporation Therapy,” in IEEE Transactions on Biomedical Engineering, vol. 62, no. 1, pp. 4-20, Jan. 2015. doi: 10.1109/TBME.2014.2367543
Miklavcic D, Davalos RV. Electrochemotherapy (ECT) and irreversible electroporation (IRE) -advanced techniques for treating deep-seated tumors based on electroporation. Biomed Eng Online. 2015;14 Suppl 3(Suppl 3):I1. doi:10.1186/1475-925X-14-S3-I1
NanoKnife. Wake Forest Baptist Health. https://www.wakehealth.edu/Treatment/n/NanoKnife. Accessed: October 15, 2019.
Sweeney DC, Neal RE, Davalos RV. Multi-scale Biophysical Principles in Clinical Irreversible Electroporation. Irreversible Electroporation in Clinical Practice. 2017:41-66. doi:10.1007/978-3-319-55113-5_3.
Images created with BioRender

Leave a comment