
Reading time: 5 minutes
Anthony Tao
In a world polarized by ethnopolitical tensions, we may be comforted to think of science as a stonewall against ethnic and social biases ‒ to imagine that scientific data speaks with an impartial voice. However, this is far from the case. The history of modern science is plagued with instances when the underrepresentation of demographics or ethnicities has led to a misguided, overgeneralization of scientific findings and clinical approaches.
A prominent example is the underrepresentation of women in clinical trials for coronary artery disease and heart attacks. Before the 1990s, the majority of such studies focused on men, with the assumption that heart disease is more severe in men than in women. In fact, the few studies that enrolled female subjects omitted the data in official reports. Following a policy change by the National Institutes of Health (NIH) that mandated better female representation in clinical investigations, subsequent studies found marked differences between the sexes in terms of heart disease presentation, progression, and even risk factors. Implementation of clinical guidelines recognizing these differences has significantly improved heart disease morbidity and mortality in women. No small feat.
In cancer research, the disparities in representation are similarly pronounced, particularly in patients of African ancestry. A recent study from 2019 has reported that only 3% of African Americans were represented in clinical trials for cancer treatments, even though they make up 14% of the US population. These numbers are concerning as African Americans suffer from higher incidences of cancer and have a worse prognosis.
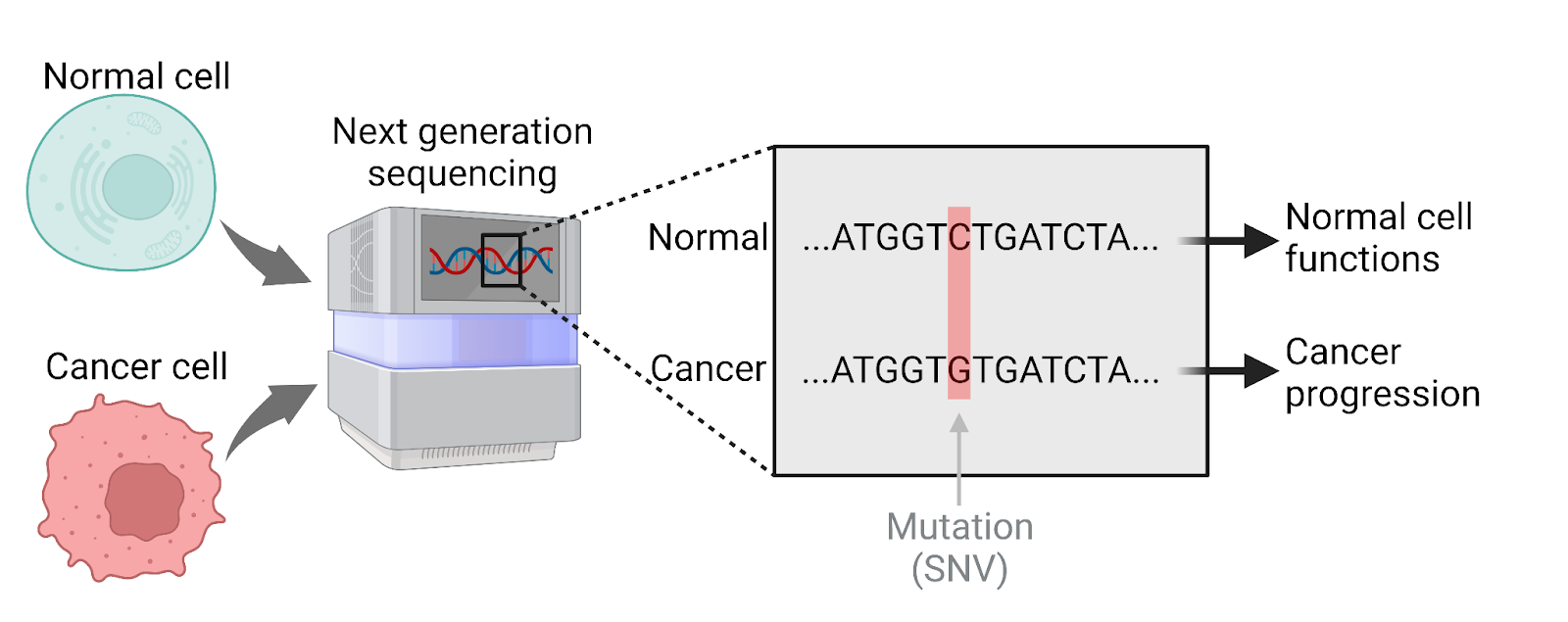
Next-generation sequencing (NGS) technology is frequently used in oncology to read the genetic information of cancer cells. It can be especially useful for finding key mutations, or changes in the genome, that drive cancer transformation and provide better insights into the molecular nature of cancer (Figure 1). NGS generates a large amount of genetic information that allows researchers to perform detailed computational analyses and devise better treatment and therapeutic approaches. Designing individual patient treatment plans guided by their genetic information is known as “personalized” or “precision” medicine. Despite significant improvements in the cost and the feasibility of NGS over the past two decades, it is still not universally accessible, especially for patients in low-income countries.
In a recent study on prostate cancer, researchers from the University of Sydney, Australia utilized NGS to gain a deeper understanding of the cancer cell genomes in patients from sub-Saharan countries in Africa. Prostate cancer patients from this region have a lower survival rate and genetic information from this demographic can lead to better and personalized cancer treatment.
The researchers used a specific form of NGS called whole-genome sequencing (WGS) to acquire detailed genetic information from the tumors of 123 cancer patients of sub-Saharan African ancestry. They further sequenced around 60 tumors from patients of European ancestry for reference. Overall, the researchers were surprised to find many mutational differences underlying African and European prostate tumors.
For instance, tumors from patients of African ancestry have a greater rate of single nucleotide variants (SNVs). To make an analogy, if the genome were a typical book, then an SNV would be similar to changing only one letter, in one word, from one page. Though minute in scale, were such SNVs to occur in important locations of the genome, like the protein-coding regions called genes, the consequences may be dire. These changes can even transform a normal cell into a cancer cell. Accordingly, the study found that mutations within African tumors occurred more frequently in the protein-coding regions, or genes, when compared to European tumors, suggesting that mutations in these regions may be more consequential.
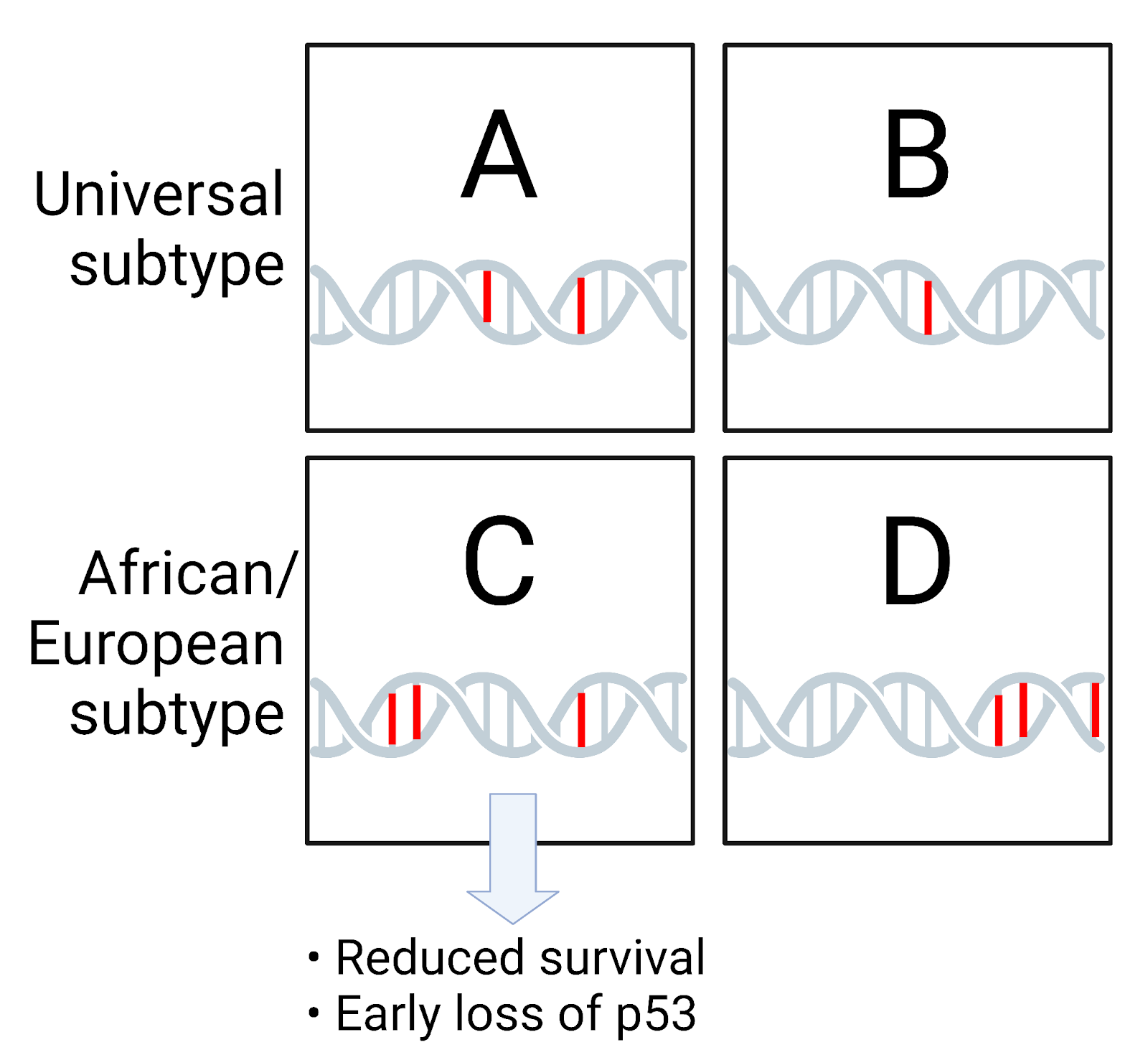
The researchers also grouped the patients based on the similarity of mutations in their tumors; this type of analysis is called molecular subtyping. They uncovered 4 subtypes of prostate cancer, designated A, B, C, and D, each having differences in progression, survival, and drug sensitivity. Subtypes B, C, and D are better represented in the prostate tumor samples from African patients than subtype A. Subtype A is a more common and universal subtype found in tumors from patients of European, African, and even Chinese ancestry. Relying on this new classification scheme, the researchers also found that patients with the universal prostate cancer (subtype A) have a better chance of survival and lower risk of relapse compared to African-specific subtype C (Figure 2). These findings demonstrate that the prevalence of prostate cancer subtypes may depend on a patient’s ancestry and can be an important determinant of patient prognosis and outcome.
Analyzing the frequencies of mutations, the researchers also determined the timing of mutations or the mutational history – that is, the order in which cancer cells acquire specific mutations. This history often differs between various cancer types and can reflect a cancer’s underlying behavior, even its aggressiveness. Using their data, the researchers discovered that the 4 subtypes of prostate cancer differ in their mutational history. For instance, in the African-specific subtype C, loss of the p53 gene ‒ a very common and powerful event in promoting cancer growth ‒ occurs earlier compared to the universal subtype A. In prostate cancer, the loss of p53 gene is associated with increased metastasis and treatment failure (Figure 2). This can explain why prostate cancer patients from sub-Saharan Africa have a worse prognosis. However, further research is required to confirm this potential causation.
NGS technology can generate large amounts of biological information rapidly and at a low cost. But, without comprehensive and robust sampling of populations, inaccurate conclusions can be easily reached. By studying patients from sub-Saharan Africa, the scientists uncovered novel mutational patterns that will allow a better classification of prostate cancers and also facilitate future investigations in the field. This study does not completely clarify if ancestral variations in prostate cancer reflect the differences in underlying genetics and geographic influences. However, this classic question of nature versus nurture is a red herring. What is important is the need for better demographic representation in NGS-oriented clinical research, especially when it comes to developing therapies for diverse patient populations. Practicing more inclusive clinical research will help precision medicine become “precise-r”.
Edited by Sneha Das

Leave a comment