Reading time: 5 minutes
Deanna MacNeil
One goal in cancer therapy is to strike a balance between treatment efficacy and toxicity. While treatments such as surgery, chemotherapy, and radiation are meant to kill cancer cells, healthy tissues can be adversely affected in the process. Common side effects of systemic cancer treatment occur because treatments work against cancer by non-specifically killing fast-growing cells. This means that some effective systemic treatments also kill non-cancer cells that divide rapidly, which leads to side effects like low white blood cell levels and hair loss. The relationship between treatment efficacy and toxicity is complex. In some instances, cytotoxic treatment side effects like reduced blood cell production and peripheral nerve damage are associated with improved treatment outcomes, while in other instances these effects have uncertain or negative associations with clinical outcomes. Importantly, many people who receive cancer treatment have a risk of developing long-term side effects months or years after treatment. Complications and long-term consequences related to treatment contribute a substantial burden to the quality of life for cancer survivors.
Individualized or personalized treatment strategies aim to maximize tumor-killing efficacy while minimizing harmful side effects by considering patient-specific characteristics such as age, genetic profile, and cancer type. Sex-specific differences in treatment efficacy and chemotherapy toxicity have been observed for decades. Yet, biological sex is rarely included in the evaluation of risks used to develop a suitable treatment regimen for a patient.
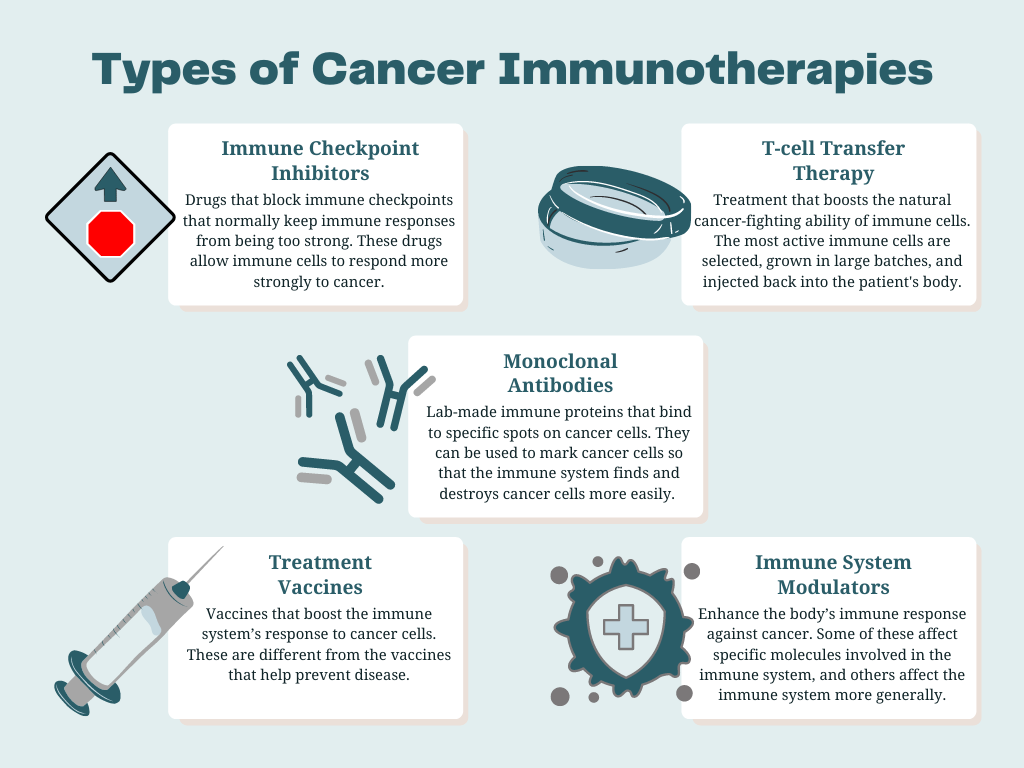
For patients with cancer, the female sex has been associated with an increased risk of negative side effects called adverse events (AEs) due to chemotherapy. However, almost no research has examined the sex-specific safety profiles of targeted therapies or immune therapies that are already being personalized. Immunotherapies are cancer treatments that help the immune system fight cancer. As part of its normal function, the immune system detects and destroys abnormal cells. Even though the immune system can prevent or slow cancer growth normally, cancer cells have ways to avoid destruction by the immune system. In cancer treatment, immunotherapy aims to influence the immune system to help it eradicate cancer cells. Immune responses vary from patient to patient, and immunotherapy cancer treatments need to be personalized for each individual patient. Sex-associated differences in the effectiveness of different immune therapies have been observed, but more information is needed to understand if and how sex affects the toxicity of immune therapies.
To bridge this gap in knowledge, a team of researchers in the United States and Canada investigated sex-specific differences in AEs caused by systemic cancer treatments, including chemotherapy with or without radiation, immunotherapy, and targeted therapy. In their study, the researchers analyzed cancer treatment-related AEs documented in phase II and phase III clinical trials from the SWOG Cancer Research Network. They examined the number of reported AEs across different cancer treatments in 23,296 patients enrolled in 202 clinical trials between 1989 and 2019. This study did not include sex-specific or sex-dominant cancers like prostate or breast cancer, so the results of this study cannot be generalized to all types of cancer. The most common types of cancer included were gastrointestinal, lung, and leukemia.
A significantly increased risk of severe toxicity with each treatment type was observed for people assigned female at birth versus people assigned male at birth. More specifically, the female sex was associated with a 34% increased risk of severe AEs. The greatest increased risk was observed for immunotherapy; the female sex was associated with a 49% increased risk of severe toxicity when receiving immunotherapy. Among all treatments, the female sex was also associated with a higher risk of experiencing 5 or more severe symptomatic AEs. This association was strongest for patients who received immunotherapy or targeted therapy.
The findings in this study support the notion that drug toxicity can be affected by biological sex, and therefore sex-specific safety consideration should be given to further individualize treatments. Major research advisory and regulatory agencies, including the NIH and FDA, have issued mandates and guidelines to better understand sex-associated differences in disease outcomes. Towards this goal, it is imperative to identify sex-related differences not only in cancer treatment efficacy but also in the safety profiles of cancer treatments.
Previous studies have identified other sex-related disparities in cancer. For example, there is a stark difference in the trends for male and female cancer incidence. The sex disparity in overall cancer incidence has narrowed over time, with the male-to-female incidence rate ratio dropping from 1.39:1 to 1.14:1 between 1995 and 2017. During this time, cancer incidence rates declined by 2% overall among people assigned female at birth versus 20% among people assigned male at birth. However, the reasons behind sex-related differences in cancer incidence are not fully understood. The sex disparities in cancer may reflect differences in environmental risk factors, hormones, or immune function.
Similarly, it is not known why sex disparities exist for cancer treatment AEs. The researchers of this study suggest that average body type differences might affect the relative dose that patients receive, and that biases may exist in the reporting or interpretation of AEs. However, this study did include a statistical adjustment based on patient body weight, as well as assessed hematologic AEs as an objective outcome. Sex-specific differences may also exist in how drugs move inside the body and how the body responds to drugs.
Sex-associated differences in immunotherapy efficacy have been reported. The findings in this study suggest that sex-related mechanisms may also affect immune therapy toxicity outcomes for patients with cancer. Further work is needed to validate the findings of this study, and to establish the causes of sex-specific toxicity outcomes. A better understanding of the underlying mechanisms could potentially lead to treatment adjustments that reduce sex-specific toxicity. Cancer treatment approaches can then be tailored with the ultimate goal of improving the personalized benefits of treatment.
Edited by Michael Marand
Header image created with Canva

Leave a comment