
Reading time: 3 minutes
Leandro de Lima Coutinho
While it would be miraculous to have a Panacea (or Elixir of Life) that would cure all diseases and prolong life, it took alchemists in the Harry Potter universe to create one. Taking a step away from fiction, it would still be incredible to have one drug that cures all types of cancer. Although the idea of a “universal remedy” seems to be the stuff of science fiction, it has already been discussed in real life. In 2015, a so-called “cancer pill” that could supposedly cure all types of cancer was being used for over 20 years as a therapy for patients in Brazil. Synthetic phosphoethanolamine (PHOS-S) was the substance that was claimed to be the cure for cancer. However, little preclinical data (such as in vitro studies of PHOS-S effects in leukemia and melanoma) were available and no clinical trials were conducted to test the efficiency of the drug. With so little data on safety or efficacy, the clinical use of PHOS-S was suspended. Various researchers then went into action to better evaluate PHOS-S in humans and, ultimately, found the claims were too good to be true.
To understand why it is very hard to develop a single drug that is able to cure all cancers irrespective of their ‘type’, we need to review some cancer biology. First, it is important to remember that the word ‘cancer’ is not related to a single disease, but to a group of diseases. According to the Instituto Nacional de Câncer (INCA) and the American Cancer Society (ACS), cancer is the name for a group of more than 100 diseases characterized by uncontrolled cellular proliferation. Thus, when we talk about ‘cancer’ we are dealing with different types of diseases; each one with its own characteristics, molecular features, and aggressiveness.
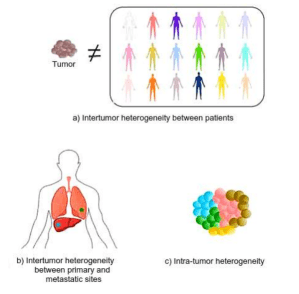
The differences between and within all cancer types are termed tumor heterogeneity and this is one reason why it is difficult to develop a single therapeutic approach to all cancer patients. Tumors from the same anatomic site, but from different patients exhibit distinctive characteristics, which is termed patient intertumor heterogeneity (Fig 1a). It makes sense that tumors from different patients have divergent characteristics, but even tumors from one patient, but different anatomic sites display unique characteristics, known as intertumor heterogeneity between primary and metastatic tumors (Fig 1b). To make it even more complicated, cancer cells from the same tumor display differences in their biology. In other words, a single tumor is composed of a variety of cell types, displaying intratumor heterogeneity (Fig 1c). So, now we can see some reasons why developing a Panacea is really unlikely in oncology. Although there is no “superpower cancer pill” available in the clinic, there are tens of thousands of researchers and clinicians around the world trying to develop and improve cancer treatment. Great progress has already been made in oncology throughout the last decades. Conservative oncology surgery, precise and accurate radiotherapy, and the improvement of chemotherapy, as well as the advances made in the targeted therapy (e.g.. trastuzumab for HER2-positive breast cancer) and immunotherapy (e.g. Nivolumab for melanoma) fields, are some of the examples that show the evolution of cancer treatment. In contrast to the idea of a ‘one-size-fits-all’ therapy for all cancers, we are now actually entering the “personalized medicine era” in which an individual’s molecular and cellular profiles are used to guide decisions made in regard to the prevention, diagnosis, and treatment of disease. All of these advances have improved oncologic patients’ welfare and cured diseases, such as certain cancers, that were once considered incurable. Ironically, as researchers and oncologists refine personalized treatments for individual cases of cancer, perhaps the need or desire for a Panacea will also go into remission.
Edited by Gabrielle Dardis
Image Credits
