Reading time: 7 minutes
Aishat Motolani
You have most likely heard of several branded FDA-approved drugs during TV commercials and sighed, “Ah! not again with this rhythmic list of symptoms.” Well, some of those symptoms may have included immune-related adverse events (IRAEs). iRAEs are composed of an array of side effects that are reminiscent of autoimmune responses. These side effects can occur in response to a class of cancer immunotherapy drugs called Immune Checkpoint Inhibitors (ICI). Although iRAEs can cause severe inflammation in several organs, multiple studies have suggested the development of iRAEs as a predictive marker for better clinical response to ICIs.
Cancer immunotherapy has been one of the most successful approaches used for cancer treatment. This is evident from the rapid expansion in the clinical development of immunotherapeutic drugs in recent years. Several of these drugs have been FDA approved for different types of cancers, including lung cancer, melanoma, bladder cancer, gastric cancer, Hodgkin’s lymphoma, etc. As notoriously known, cancerous cells have many talents— one of which is avoiding immune system surveillance. Suppressing the action of the immune system allows tumor cells to display rapid cell growth, cell migration and invasion, limitless replication, formation of new blood vessels, and insensitivity to anti-growth signals. These features are collectively known as hallmarks of cancer.
To better understand cancer cells’ prowess in escaping immune surveillance, let us briefly review the immune system. The immune system is made up of different specialized cells that circulate throughout the body or reside in a specific organ to protect the body from any foreign particles or disease-causing organisms (pathogens). Simply put, the immune system differentiates self from non-self and works tirelessly to eliminate the non-self.
Based on the speed and specificity of response, the immune system is classified into the innate and the adaptive immune system. The ever-so-swift innate immune system is considered the first line of defense during an immune response. It includes physical barriers such as the skin, chemical barriers such as mucus and tears, and immune cells such as neutrophils, macrophages, natural killer cells, etc. On the other hand, the adaptive immune system is slower but more specific, and it is composed of T-cells and B-cells. During the adaptive immune response, a fraction of a non-self entity, known as an antigen, is presented to particular T-cells and B-cells to activate them. Once activated, the T-cells and B-cells rapidly multiply. The B-cells produce antibodies and recruit T-cells and other immune cells to eliminate the pathogen. Antibodies increase the visibility of a pathogen or foreign substance to the immune system. This can be likened to the use of a muleta by a bull-fighter to mobilize a bull.
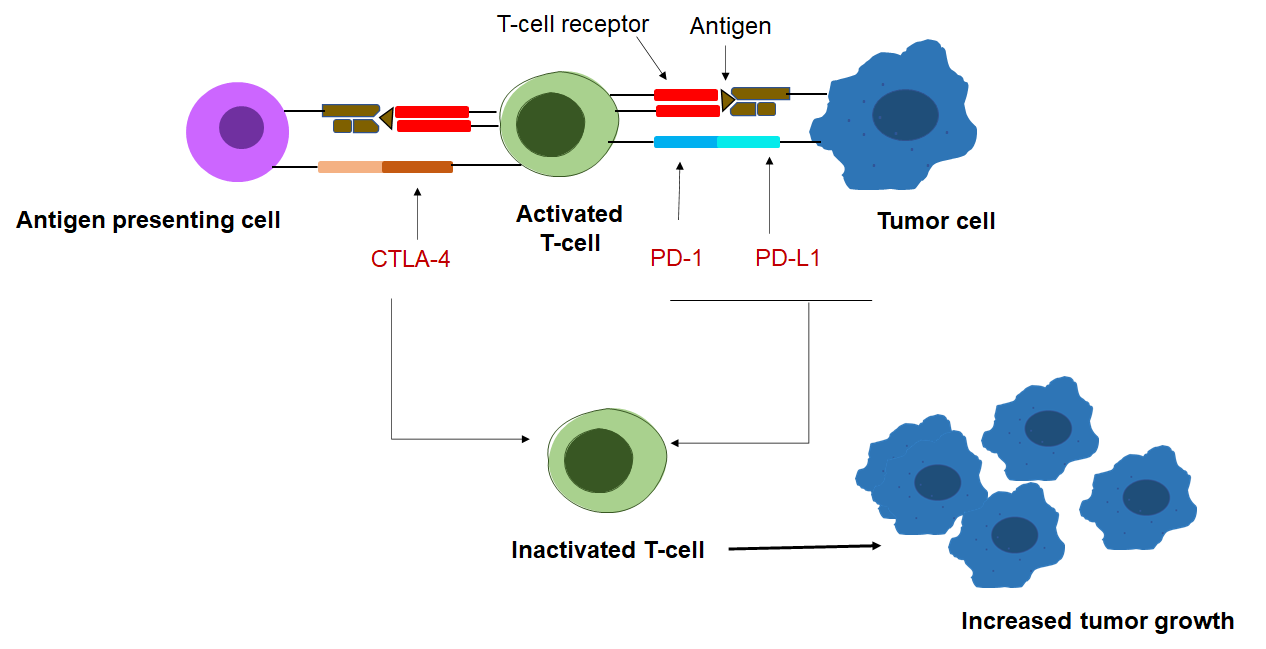
In cancer, various specialized immune cells reside in the surrounding area of tumor cells (the tumor microenvironment). The particular immune cell of interest to cancer immunotherapy researchers is the T-cell because it exclusively champions cancer immunity. In a healthy individual, when a threat is detected— let’s say a virus— two things need to occur for T-cell activation. First, an antigen-presenting cell (APC) detects the antigen and offers the virus antigen to the T-cell receptor. Second, a lock-and-key interaction occurs between proteins on the APC and the T-cell to fully activate the T-cell into a raging defender. In cancer, tumor cells often prevent the second step from happening by upregulating immune checkpoint proteins, thereby creating an immunosuppressive system in an individual. Also, since a tumor cell arises from genetically altered cells in the body, it is difficult for the immune system to recognize it as a threat and consider it as non-self. This difficulty in recognition is caused by a process called cancer immunoediting. In this process, the innate and adaptive immune systems work together to eliminate tumor cells that strongly express tumor-specific antigens before the tumor cells manifest clinically as cancer. Then, in the equilibrium phase, the tumor cells that were not eliminated become dormant and undergo editing to become resistant to immune cells. This process allows tumor cells to escape further immune attacks.
Where do ICIs fit into this tug of war between tumor cells and immune cells? Immune checkpoint proteins function to suppress hyperactivity of immune cells, which may cause an autoimmune attack on the body’s healthy cells. Tumor cells hijacked this function to ensure their survival amidst T-cells’ constant attempted assault. During the equilibrium phase, tumor cells recruit immune cells such as Treg, which constantly express these immune checkpoint proteins. Additionally, tumors increase the expression of immune checkpoint proteins on their own surface and on antigen-presenting cells to deactivate any killer T-cell encountered. The most studied immune checkpoint proteins are cytotoxic T-lymphocyte-associated antigen 4 (CTLA4), programmed cell death protein 1 (PD1), and programmed cell death-ligand 1 (PD-L1). In cancer, these proteins actively work to limit the elimination of tumors by inactivating T-cells. Hence, immune checkpoint inhibitors—such as anti-PD1, anti-PD-L1, or anti-CTLA4—function to boost T-cell function and cancer immunity.
To date, about six ICIs have been approved by the FDA, including ipilimumab, Nivolumab, Pembrolizumab, Avelumab, and Durvalumab. Cancer patient treatment response rates with these ICIs range from 15% to 60%. But, despite the glimmering success of immune checkpoint inhibitors, like every drug, they can cause adverse side effects and toxicity. So, although ICIs are directed towards enhancing tumor immunity, they may also activate non-specific tumor immune responses that cause harm to healthy tissues. This occurrence is described as iRAEs. Some examples of iRAEs include thyroiditis, rheumatoid arthritis, hepatitis, and myocarditis. iRAEs often develop in cancer patients within 2 to 16 weeks of receiving ICI treatment, and the management of iRAEs is typically dependent on the organ of occurrence and the severity of iRAEs.
Besides the toxicities caused by iRAEs in response to immune checkpoint drugs, a growing body of evidence has proffered an optimistic perspective that iRAEs can be used as a measure of ICIs’ response. For instance, in retrospective studies (studies that look back on past events) examining lung cancer patients, it was reported that in patients who received anti-PD-1 and PD-L1 drugs, those who experienced iRAEs exhibited significantly increased disease-free survival and overall survival compared to those who did not have iRAEs. In another retrospective study conducted with 576 melanoma patients, there was a significant overall response rate in patients who developed iRAEs compared to those that did not develop iRAEs after nivolumab treatment. Similarly, retrospective analysis of renal cell carcinoma patients treated with immune checkpoint drugs demonstrated the development of iRAEs is associated with the overall survival rate. Several other studies have reported a similar positive correlation between iRAEs onset induced by anti-PD-1 and PD-L1 drugs with overall response rate, disease-free survival, or overall survival in head and neck cancers, urothelial carcinoma, and gastrointestinal cancers. Interestingly, this positive correlation is not as consistent in studies with anti-CTLA-4 drugs. Multiple retrospective studies in melanoma patients receiving anti-CTLA-4 drugs showed either a positive correlation or no difference in patients who developed iRAEs in response to ICI treatment and their overall survival rate.
The predictive ability of iRAEs on ICIs’ effectiveness may not be clear-cut and can be muddled by a variety of factors. Some of these factors include the duration of ICI treatment, the timing of iRAEs onset, the site of iRAE development, the severity of iRAEs, and management of iRAEs with anti-inflammatory steroids. Although the discussed correlation between iRAEs and ICI suggests the use of iRAEs as a measure of ICIs’ response, it does not alleviate the associated toxicities and discomfort caused by the developed iRAEs. So, the key to maximizing the ability of ICIs to enhance anti-tumor immunity is to discover a way to uncouple the blessings associated with iRAE from its curse.
Edited by Michael Marand
Works Discussed
Haslam A, Prasad V. Estimation of the Percentage of US Patients With Cancer Who Are Eligible for and Respond to Checkpoint Inhibitor Immunotherapy Drugs.(2019). JAMA Netw Open. 2(5):e192535. doi:10.1001/jamanetworkopen.2019.2535
Hanahan, D., & Weinberg, R. A. (2000). The hallmarks of cancer. Cell, 100(1), 57–70. https://doi.org/10.1016/s0092-8674(00)81683-9
Parkin, J., & Cohen, B. (2001). An overview of the immune system. The Lancet, 357(9270), 1777-1789.
DuPage, M., Mazumdar, C., Schmidt, L. M., Cheung, A. F., & Jacks, T. (2012). Expression of tumor-specific antigens underlies cancer immunoediting. Nature, 482(7385), 405–409. https://doi.org/10.1038/nature10803
Pardoll, D. (2012).The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer 12, 252–264 https://doi.org/10.1038/nrc3239
Michot, J. M., Bigenwald, C., Champiat, S., Collins, M., Carbonnel, F., Postel-Vina
y, S., … & Lambotte, O. (2016). Immune-related adverse events with immune checkpoint blockade: a comprehensive review. European journal of cancer, 54, 139-148.
Shankar, B., Zhang, J., Naqash, A. R., Forde, P. M., Feliciano, J. L., Marrone, K. A., … & Naidoo, J. (2020). Multisystem Immune-Related Adverse Events Associated With Immune Checkpoint Inhibitors for Treatment of Non–Small Cell Lung Cancer. JAMA oncology, 6(12), 1952-1956.
Das, S., & Johnson, D. B. (2019). Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. Journal for immunotherapy of cancer, 7(1), 1-11.

Leave a comment